|
ABNORMAL WAVEFORMS IN
THE UTEROPLACENTAL
CIRCULATION |
The process of trophoblastic invasion develops at about 8 weeks gestation and is well established by 18 weeks. During this process the spiral artery is converted into a low resistance high conductive vessel. This is paralleled by the progressive increase in end diastolic velocities in the arcuate arteries from 14-20 weeks gestation, with no change thereafter.
Campbell and co-workers (1) examined 126 singleton pregnancies. They analyzed the arcuate arterial flow velocity waveform at 18 weeks in an attempt to predict pregnancy induced hypertension, IUGR and fetal hypoxia.
- 64% of hypertensive pregnancies were correctly predicted.
- 66% of growth retarded fetuses were correctly predicted.
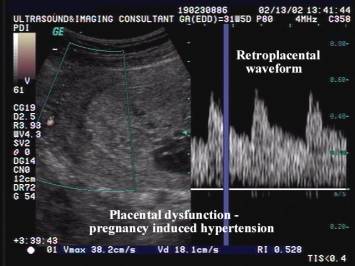
The importance of examining the uteroplacental blood flow is that a normal pattern in the presence of abnormal umbilical artery resistance indices suggests that the primary defect is probably on the fetal side of the placenta. Abnormal umbilical and uteroplacental flow velocity waveforms represent a group in which vascular disease exists in the uteroplacental vascular bed. Uteroplacental waveforms have been used to assess the effectiveness of therapy in patients with acute hypertension and preeclampsia (2,3).

REFERENCES
|
- Campbell S, Pearce JMF, Hackett G et.al. Qualitative assessment of uteroplacental blood flow: early screening test for high risk pregnancies. Obstet Gynecol 1986;68:649.
- Pritchard JA, MacDonald PTC. Hypertensive disorders in pregnancy. In: Pritchard JA, MacDonald PTC (eds). Williams Obstetrics (17th ed). New York, Appleton-Century-Crofts 1985:525.
- Fairlie FM. Doppler flow velocimetry in hypertension in pregnancy. Clinics in Perinatology 1991;18:749-778.